What Is Radiating Shoulder Pain?
When pain does not stay in the shoulder but travels down the arm, we are dealing with referred pain. In many people this is linked to irritation or compression of the cervical nerve roots (radiculopathy), causing pain to follow a specific path along the arm — sometimes felt as an electric shock, numbness or loss of strength.
Unlike a purely muscular injury, this condition suggests something is compromising the passage of nerve signals or circulation — whether at the exit of the cervical spine, at the passage through the clavicle (thoracic outlet) or beneath the chest and shoulder muscles.
This feeling of a “heavy” arm, tingling or electric shocks is a sign that the nervous system is more sensitive and under mechanical tension — particularly with movements like stretching the arm out, turning the head, or reaching for objects.
My Clinical View
The arm is the end of the line, not the origin
Very often, the pain you feel in your bicep or forearm is simply the “echo” of a problem in the neck or first rib. In clinical practice, it makes more sense to evaluate the entire nerve path — cervical spine, shoulder and rib cage — rather than treating only the point that hurts.
The goal is not to “push through” until the arm stops hurting, but to restore mobility to the joints and tissues surrounding the nerve, so that it can glide again with less irritation and the pain stops projecting along the upper limb.
Symptomatic Treatment (Medication)
Relying on anti-inflammatories focuses only on “switching off” the symptom.
- Temporary Solution: Useful only in very acute phases.
- Cause Remains: The nerve stays compressed due to lack of space or stiffness.
- Pain Cycle: The symptom returns as soon as the medication wears off.
Neurodynamic Approach (TrataMentes)
We work to reduce mechanical irritation and improve nerve gliding.
- Plexus Release: We create space in the rib cage and shoulder for the nerve to pass freely.
- Neurodynamic Techniques: We restore nerve mobility.
- Gentle Mobilisation: We increase movement tolerance without forcing.
Relying on anti-inflammatories focuses only on “switching off” the symptom.
- Temporary Solution: Useful only in very acute phases.
- Cause Remains: The nerve stays compressed due to lack of space or stiffness.
- Pain Cycle: The symptom returns as soon as the medication wears off.
We work to reduce mechanical irritation and improve nerve gliding.
- Plexus Release: We create space in the rib cage and shoulder for the nerve to pass freely.
- Neurodynamic Techniques: We restore nerve mobility.
- Gentle Mobilisation: We increase movement tolerance without forcing.
Common Causes of Radiation
Origins of Compression
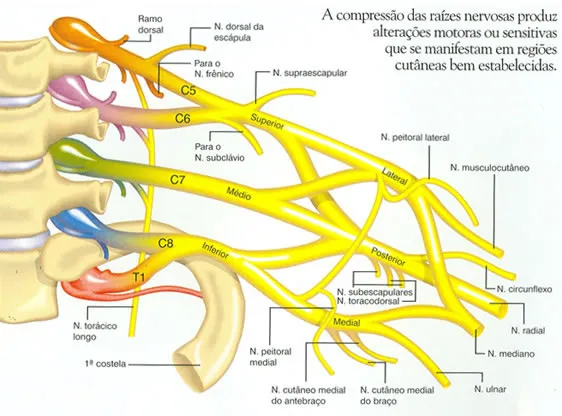
- Cervical Radiculopathy: Irritation or compression of a nerve root at the base of the neck (for example C5, C6, C7), sending pain, tingling or weakness along a specific path in the arm.
- Thoracic Outlet Syndrome: Compression of nerves and vessels between the clavicle and the first rib, which can cause numbness, a sensation of heaviness or colour changes in the hand — especially on the inner side of the arm and fingers 4 and 5.
- Trigger Points: Deep muscular knots in muscles such as the infraspinatus or scalenes, which project pain at a distance and can mimic nerve pain without significant root compression.
- Increased Neurodynamic Tension: The nerve loses its ability to glide comfortably during movement, generating symptoms when you extend the arm, rotate the neck, or hold certain postures for a prolonged period.
Red Flags
Seek specialist assessment urgently if you notice:
- Clear loss of strength: Beginning to drop objects, obvious difficulty lifting the arm or gripping.
- Constant and extensive numbness: Loss of sensation that does not improve with position changes or that spreads rapidly up the arm.
- Colour changes or hand swelling: Hand very pale, purplish, cold or with sudden oedema — which may suggest vascular compromise in the thoracic outlet.
- Persistent and debilitating night pain: Pain that wakes you repeatedly and does not ease with small position changes, especially if combined with fever, weight loss or recent trauma.
How Manual Therapy Helps
To treat radiation, we use a progressive and functional decompression approach, integrated with specific exercises:
- Cervical and Thoracic Mobilisation: Gentle, gradual movements to improve mobility of the cervical vertebrae and the mid-back region, creating relative space for the nerve roots to pass and reducing the nociceptive stimulus.
- Neurodynamic Techniques: Passive and active movements that allow the nerve to “glide” between tissues (for example, for the median, radial or ulnar nerve), helping to reduce sensitivity and improve conduction without increasing pain.
- Release of Key Muscles (such as Pectoralis Minor and Scalenes): Specific work in these regions can reduce compression on the brachial plexus at the thoracic outlet, improving circulation and symptoms in the arm.
Studies show that adding neural mobilisation to a physiotherapy/conservative therapy plan can improve pain, cervical mobility and upper limb function in people with cervical radiculopathy — particularly when integrated within an exercise and postural education programme.
Assess the Arm Tension
Functional diagnostic consultation in Lisbon or Cascais
Book Your Session Nowor call +351 937 543 312
The Road to Recovery
Typical Results
- Reduction in the intensity and frequency of electric shocks and tingling in many mild-to-moderate cases.
- Gradual improvement in neck mobility and less feeling of “locking” when turning the head.
- Partial relief of the “heaviness” sensation in the arm, especially at rest.
- Reduction in the intensity and frequency of electric shocks and tingling in many mild-to-moderate cases.
- Gradual improvement in neck mobility and less feeling of “locking” when turning the head.
- Partial relief of the “heaviness” sensation in the arm, especially at rest.
- Continued recovery of grip strength and confidence in using the arm day to day.
- Pain more localised at the point of origin (neck/shoulder), with less radiation to the hand.
- Progressive return to activities such as driving, computer work and household tasks with less limitation.
- Continued recovery of grip strength and confidence in using the arm day to day.
- Pain more localised at the point of origin (neck/shoulder), with less radiation to the hand.
- Progressive return to activities such as driving, computer work and household tasks with less limitation.
- In many cases, radiation becomes rare or disappears, with only some residual sensitivity under greater effort.
- Greater nerve tolerance to load, impact and prolonged positions, thanks to strengthening and movement re-education.
- Gradual and safe return to sport and heavier professional tasks, with a maintenance plan to prevent recurrence.
- In many cases, radiation becomes rare or disappears, with only some residual sensitivity under greater effort.
- Greater nerve tolerance to load, impact and prolonged positions, thanks to strengthening and movement re-education.
- Gradual and safe return to sport and heavier professional tasks, with a maintenance plan to prevent recurrence.
Typical Results
- Reduction in the intensity and frequency of electric shocks and tingling in many mild-to-moderate cases.
- Gradual improvement in neck mobility and less feeling of “locking” when turning the head.
- Partial relief of the “heaviness” sensation in the arm, especially at rest.
- Reduction in the intensity and frequency of electric shocks and tingling in many mild-to-moderate cases.
- Gradual improvement in neck mobility and less feeling of “locking” when turning the head.
- Partial relief of the “heaviness” sensation in the arm, especially at rest.
- Continued recovery of grip strength and confidence in using the arm day to day.
- Pain more localised at the point of origin (neck/shoulder), with less radiation to the hand.
- Progressive return to activities such as driving, computer work and household tasks with less limitation.
- Continued recovery of grip strength and confidence in using the arm day to day.
- Pain more localised at the point of origin (neck/shoulder), with less radiation to the hand.
- Progressive return to activities such as driving, computer work and household tasks with less limitation.
- In many cases, radiation becomes rare or disappears, with only some residual sensitivity under greater effort.
- Greater nerve tolerance to load, impact and prolonged positions, thanks to strengthening and movement re-education.
- Gradual and safe return to sport and heavier professional tasks, with a maintenance plan to prevent recurrence.
- In many cases, radiation becomes rare or disappears, with only some residual sensitivity under greater effort.
- Greater nerve tolerance to load, impact and prolonged positions, thanks to strengthening and movement re-education.
- Gradual and safe return to sport and heavier professional tasks, with a maintenance plan to prevent recurrence.
* Results vary depending on severity, chronicity, and treatment adherence.
Note: These timelines are averages observed across many people with well-guided conservative treatment; some cases improve faster and others may need more time — especially when nerve compression is more longstanding or severe.
Decompression Exercises (For Home)

Median Nerve Glide
10 gentle oscillations · 3x per dayMedian Nerve Glide
Exercício
Chin Tuck
12 repetitions · 3x per dayChin Tuck
Exercício
Pectoral Self-Release
1 minute · 1x per dayPectoral Self-Release
ExercícioScientific Evidence
Scientific References
Basson, A., Olivier, B., Ellis, R., Coppieters, M., Stewart, A., & Mudzi, W. (2017). The effectiveness of neural mobilization for neuromusculoskeletal conditions: A systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 47(9), 593–615.
Rafiq, S., Rafique, Z., Ahmed, A., et al. (2022). Comparison of neural mobilization and conservative treatment on pain, range of motion and disability in cervical radiculopathy: A randomized controlled trial. PLOS ONE, 17(12), e0278177.
López-Pardo, M. J., et al. (2024). Routine physical therapy with and without neural mobilization on pain and mobility in chronic cervical radiculopathy. Archives of Medical Science.
Savva, C., et al. (2013). The effect of cervical traction combined with neural mobilization on pain and disability in a patient with cervical radiculopathy. Manual Therapy.
Savva, C., et al. (2016). Effectiveness of neural mobilization with intermittent cervical traction in patients with cervical radiculopathy: A randomized clinical trial.
Scientific References
Basson, A., Olivier, B., Ellis, R., Coppieters, M., Stewart, A., & Mudzi, W. (2017). The effectiveness of neural mobilization for neuromusculoskeletal conditions: A systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 47(9), 593–615.
Rafiq, S., Rafique, Z., Ahmed, A., et al. (2022). Comparison of neural mobilization and conservative treatment on pain, range of motion and disability in cervical radiculopathy: A randomized controlled trial. PLOS ONE, 17(12), e0278177.
López-Pardo, M. J., et al. (2024). Routine physical therapy with and without neural mobilization on pain and mobility in chronic cervical radiculopathy. Archives of Medical Science.
Savva, C., et al. (2013). The effect of cervical traction combined with neural mobilization on pain and disability in a patient with cervical radiculopathy. Manual Therapy.
Savva, C., et al. (2016). Effectiveness of neural mobilization with intermittent cervical traction in patients with cervical radiculopathy: A randomized clinical trial.