What Is It?
Shoulder pain when lifting your arm is one of the most common signs of shoulder dysfunction. It appears when you raise your arm overhead — reaching a shelf, dressing, combing your hair, or during sport movements.
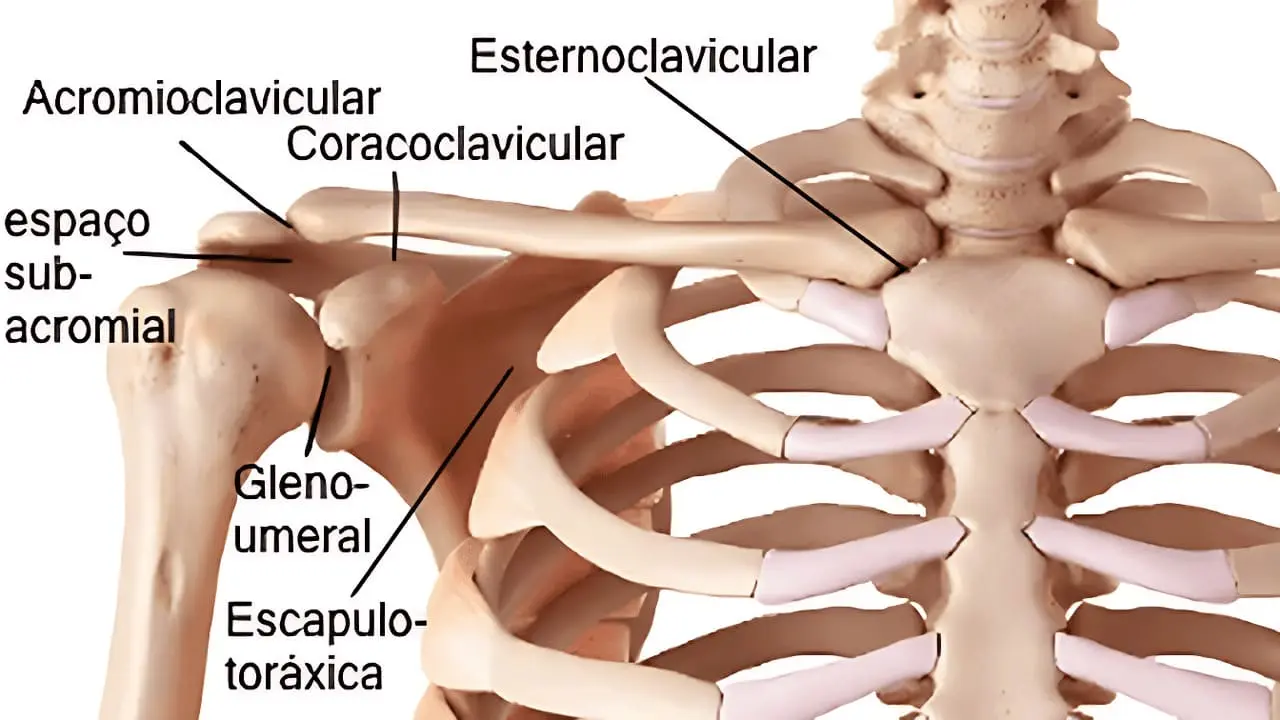
Clinically it is called Subacromial Pain Syndrome (SAPS): irritation of the tendons and soft tissues trapped between the acromion (shoulder bone) and the head of the humerus. As the arm rises, the space narrows and those structures get compressed — causing pain.
This is one of the most frequent reasons people seek shoulder treatment, affecting all ages from athletes to office workers.
When It Appears and Common Signs
Recognise whether this is what you feel:
- Pain when raising the arm to a shelf or cupboard
- Discomfort when combing your hair or washing your head
- Difficulty dressing — pulling on jumpers or jackets
- Discomfort during overhead exercise (weight-lifting with arm extended)
- Pain when sleeping, especially lying on the affected shoulder
- Morning stiffness when you wake up
- Painful arc — a specific range (usually 60–120°) where movement hurts most
Pain typically sits on the side or front of the shoulder and may radiate down the arm. It often starts gradually with no specific injury and worsens over weeks or months.
Possible Causes
This type of pain usually results from a combination of factors:
Structural factors
- Supraspinatus tendinitis (one of the rotator cuff tendons)
- Subacromial bursitis (fluid-filled sac that cushions shoulder movement)
- Muscular contractions in the scapular stabilisers
- Poor scapular stability
- Reduced subacromial space due to postural changes
Biomechanical factors
- Muscle imbalance between shoulder muscles (weak external rotators)
- Weakness of the mid and lower trapezius
- Postural misalignment (elevated or protracted shoulders)
- Inadequate working positions held for long periods
- Poor scapulohumeral coordination (desynchronised movement between scapula and humerus)
Overload factors
- Repetitive overhead work with the arm raised
- Intensive training without adequate recovery
- Long hours sitting at a computer
- Repetitive overhead movements (painters, swimmers, tennis players)
- Carrying loads incorrectly
The key point: This rarely means serious structural damage. Most cases are accumulated overload combined with reduced mobility and stability. With the right treatment, recovery is very common.
Positions and Movements That Worsen Pain
Pain typically worsens with:
- Elevation movements: lifting the arm, especially between 60° and 120° of abduction
- Overhead activities: throwing, swimming, painting ceilings
- Night positions: lying on the affected shoulder
- Prolonged computer work: increased neck and scapular tension
- Lifting with load: carrying weights with the arm extended
- Reaching behind the back: putting on a jacket, reaching for a wallet
- Pushing or pulling heavy objects
There is often a “painful arc” — a specific range of motion where pain peaks, easing when the arm moves past that angle.
When to Be Concerned
Medical Red Flags
Seek medical assessment immediately if you experience:
- Intense sudden pain after a fall or impact.
- Complete inability to lift your arm.
- Significant swelling or colour change.
- Fever, intense heat or redness (signs of infection).
- Numbness or tingling running down the arm.
- Progressive weakness preventing movement.
- Visible deformity at the joint.
- No improvement after 2 weeks of self-care.
Positive Note
How Therapeutic Massage and Manual Therapy Can Help
The goal is to reduce pain, restore full mobility and re-establish efficient movement patterns.
What we do:
1. Release muscular tension
- Therapeutic massage techniques to loosen contracted muscles of the shoulder and neck
- Work on the upper trapezius, pectoral and scapular stabilisers
- Reducing contractions that block movement
- Soft tissue techniques to improve circulation
2. Joint mobilisation
- Glenohumeral joint mobilisation techniques to restore range of motion
- Scapular work to improve scapular dynamics
- Release of impingement through controlled movements
- Restoration of scapulohumeral rhythm
3. Tendon treatment
- Tendon gliding techniques
- Stimulating blood flow to accelerate recovery
- Progressive work within the tolerance zone
- Reducing inflammation through specific techniques
4. Postural and movement re-education
- Correcting inadequate postural patterns
- Scapular stabilisation training
- Learning efficient movement patterns
- Motor control exercises
5. Breathing work
- Neck and shoulder relaxation through diaphragmatic breathing
- Integrating breathing with movement
- Reducing upper thoracic tension
Expected outcome
Pain begins to ease within the first sessions and mobility improves progressively over days. Most clients experience significant relief in 4 to 8 sessions, depending on severity and chronicity.
When to Refer to a Specialist
I work in coordination with other health professionals. I may refer you to:
- GP or orthopaedic surgeon: if there is suspicion of serious structural damage (tendon rupture, labral injury, etc.)
- Radiology: for imaging (ultrasound or MRI) if needed
- Physiotherapist: for complementary rehabilitation and supervised progressive exercise
- Sports medicine doctor: for athletes with specific requirements
The good news: Recent high-quality research shows that subacromial decompression surgery offers no additional benefit over conservative treatment (massage, manual therapy + exercise) for pain and function in most cases⁹.
What to Expect from a Session
First assessment (45–60 minutes)
- Detailed interview about pain history
- Mobility and strength tests
- Postural and movement pattern assessment
- Identification of specific restrictions
- Personalised treatment plan
Treatment sessions (30–45 minutes)
- Massage and muscular release techniques
- Joint mobilisation
- Stabilisation exercises
- Home guidance
Between sessions
- Specific stretches and exercises
- Postural modifications in daily life
- Gradual activity progression
- Self-massage with ball or foam roller, if appropriate
Typical Results and Timelines
Short term (1–2 weeks)
- 30–50% reduction in pain
- Improved sleep quality
- Slight increase in range of motion
- Reduced morning stiffness
Medium term (4–8 weeks)
- Significant pain relief (70–80% in many cases)
- Full functional recovery for daily activities
- Gradual return to exercise
- Improved stability and motor control
Long term (8–12 weeks)
- Complete resolution in uncomplicated cases
- Return to overhead activities without restrictions
- Reduced recurrence risk through maintenance exercise
- Integration of new movement patterns
Influencing variables
- Initial severity: the more severe, the more time may be needed
- Duration of symptoms: the more chronic, the longer recovery may take
- Adherence to home exercises: essential for optimal results
- Postural habits at work: modifications needed to prevent recurrence
- Age and general physical condition: influence recovery capacity
Scientific Evidence
This type of pain is well documented in international scientific literature. Here is the evidence on the effectiveness of conservative treatment:
Diagnosis and prevalence
- Subacromial Pain Syndrome accounts for 44–65% of shoulder complaints in medical consultations¹
- It affects athletes and people with repetitive overhead work²
Mechanism
- Involves muscle imbalance with weakness of the external rotators and mid/lower trapezius³
- Scapular misalignment increases subacromial compression⁴
Effectiveness of manual therapy, mobilisation and exercise
- Multiple systematic reviews show that manual therapy combined with exercise significantly reduces pain⁵
- Meta-analysis shows that the combination of manual therapy + exercise is superior to either treatment alone⁶
- Randomised controlled trials confirm manual therapy reduces pain by 40–50% in 4–8 weeks⁷
- Research shows that joint mobilisation techniques improve shoulder function by up to 30%⁸
Comparison with surgery
- Critical finding: High-quality studies show that subacromial surgical decompression offers NO additional benefit over conservative treatment (massage, manual therapy + exercise) for pain and function⁹
- Conservative treatment delivers outcomes comparable to surgery, without the risks of invasive procedures
Combined treatment is more effective
- The combination of manual therapy with exercise shows superior results to either treatment alone¹⁰
Scientific references
¹ NCBI – Shoulder Impingement Syndrome (2023) – StatPearls ² Cleveland Clinic – Shoulder Impingement ³ International Journal of Sports Physical Therapy (2011) ⁴ PMC – Subacromial Pain Syndrome Guideline – Dutch Orthopaedic Association ⁵ JOSPT – Systematic Review of Conservative PT Interventions (2020) ⁶ PMC – Manual Therapy and Exercise for Rotator Cuff (2024) ⁷ PMC – Effectiveness of Manual Physical Therapy for Shoulder Conditions (2009) ⁸ AAOS – Shoulder Impingement/Rotator Cuff Tendinitis ⁹ PMC – Subacromial Impingement Syndrome: Medical Myth? (2022) ¹⁰ ScienceDirect – Shoulder Pain Treatment Guideline
Complementary Exercises (to do at home)
Important: These exercises should be done without pain. If you feel pain, stop and seek professional guidance.
1. Chest stretch (2x/day)
Place your arm in a door frame (elbow at 90°) and rotate your body to the opposite side. Hold for 30 seconds.
2. Scapular retraction (3x/day, 10 repetitions)
Sitting upright, squeeze your shoulder blades back and down, as if trying to hold a pencil between them.
3. Controlled wall slide (2x/day, 10 repetitions)
Standing next to a wall, slide your arm up the wall while keeping your scapula stable.
4. External rotation with resistance band (1x/day, 15 repetitions)
With your elbow tucked to your side, pull the resistance band outwards, strengthening the external rotators.
Related Reading
Also explore these related symptoms for a more complete picture:
Book Your Assessment
If you have shoulder pain when lifting your arm and want to recover your quality of life, book a no-commitment assessment.
Locations:
- Lisbon – Alvalade (Rua Jorge Colaço 11B)
- Cascais
Last updated: 15 January 2025